15 YEAR OLD MALE WITH ACUTE KIDNEY INJURY.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
Presenting complaints :
A 15 yr old male ,studying 9 th class came to the casuality with C/O SOB( grade 2 - 3 ) since yesterday ,orthopnea +
HOPI :
Pt was apparently asymptomatic 1 month back ,pt complains of vomitings 2 - 3 episodes daily associated with food particles not associated with blood ,for around 1 month
H/O fever 1 month back associated with chills ,relieved with medication by 2 days
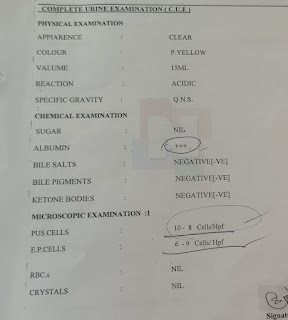
InIncidentally patient found to have urea 62 mg/dl
Creatinine 8.3 went to Hyderabad within 1 day urea has raised to 135mg/dl and creatinine 10.7
And started him on dialysis .5 sessions of HD done and USG abdomen showing B/L kidneys size of 8.1 cms Grade 3 RPD changes .Since then he was on hemodialysis pt C/O SOB since yesterday evening aggravating on supine position Grade 2 - 3 ,not associated with PND
C/O chest pain ,dragging type only during episode of sob
No C/O palpitations ,syncope attack
No C/O decreased urine output ,pedal edema ,facial puffiness
Previous reports :



Past History:
Hypertensive since 1 month and is on Tab.AMLONG 5 mg
History of 3 transfusions 1 month back
Not a K/C/O DM ,Asthma ,epilepsy ,thyroid disorders
Family History :
No H/O renal problems in their whole family.
His paternal grandfather is diabetic and hypertensive
Personal History:
Diet - mixed
Appetite - normal
Sleep - adequate
Bowel movements : regular
Bladder movements : regular
No history of alcohol consumption or smoking history
General Examination:
Patient is conscious, coherent , cooperative
Pallor -present
Icterus -absent
Clubbing-absent
Cyanosis -absent
Generalised Lymphadenopathy-absent
Pedal Edema -absent
O/E:
Vitals:
On day 1
Temperature : 98.6°F
BP: 140/90 mm Hg in right upper arm in supine position
PR: 76 bpm
RR: 20 cycles per minute
Spo2: 88% on room air
96% at 4 litres of O2
Vitals :
Temperature : afebrile
Pulse rate : 96 bpm
Respiratory rate : 24 cycles /min
BP : 140/100 mm of Hg
SpO2 : 86 % at Room air .
GRBS : 121 mg%
Systemic Examination:
CVS: S1,S2 heard no murmurs
CNS: normal
RS :
Bilateral Air Entry - present
Bilateral crepitations heard at IAA and ISA.
No wheeze .
PA:
Soft ,non tender
Bowel sounds +
CNS:
NAD
Investigations :
On day 1





Tachypnoea :
ECG report :


Provisional diagnosis : Acute Kidney Injury (AKI) secondary to ? PSGN ? IgA nephropathy ? Minimal change disease
Treatment :
On day 1
1. Tab Lasix 40mg po/ BID
2. Neb with duolin ,budecort -8th hourly
3.Tab .Zoffer - 4mg po /TID
4. Tab .Nodosis -500mg po /BID
5. O2 inhalation to maintain SpO2
6. Tab orofer AT po /BID
7.STRICT I/O CHARTING
8. BP ,PR,RR CHARTING
9. Tab Rantac 150 mg po /OID
Comments
Post a Comment