65 year old male with anasarca
65 YEAR OLD MALE WITH ANASARCA
65 year old male came to the casuality on at 3:30pm on 8/11/21
with
c/o b/l pedal edema since 10 days
c/o shortness of breath since 4 days
c/o facial puffiness since 2 days
c/o decreased appetite since 2 days
c/o decreased urine output
Patient was apparently asymptomatic 3 years ago, then he developed Rt sided hemiparesis and was diagnosed with CVA and was on antiplatelets on and off.
He was also diagnosed with DM at that time and HTN one year later
Patient has c/o pedal edema ( upto knee, decreasing on rest ) and shortness of breath ( grade II-III ) since 1 1/2 year and was diagnosed with chronic kidney disease 1 1/2 years ago and is on regular medication.
No dialysis was done. Managed conservatively.
C/o pedal edema since 10 days gradually progressed toward face
(Pitting type)
C/o shortness of breath (grade II-III)
since 4 days
Facial puffiness since 2 days
A/w loss of appetite and decreased urine output
Not a/w orthopnea, PND
The patient has been married for 31 years and has two daughters (30 yrs and 26 yrs). He is a Village revenue officer by occupation.
He used to go to work everyday and was able to perform all his daily activities on his own. Even after his CVA which caused rt hemiparesis 3 years ago, he used to go to work everyday post his recovery
But since about 1 1/2 year ago he is not able to go to work regularly due to his swollen
feet and has been going to work only when he had meetings to attend. He completely stopped going to work since the past few months.
Even during this time he was able to perform his day to day activities at home on his own until 10 days ago when he started
developing extensive swelling, staring in his feet, gradually progressing to his entire body when he couldn’t even stand up on his own and needed help from a family member for all his daily activities.
Even his speech became unclear since the past few days.
K/C/O
DM since 3 years - on human actrapid
15U——x——-8U
HTN since 11/2 year- on Tab. Met XL
CAD
Personal:
Diet-mixed
Appetite - reduced
Sleep - reduced
Bowel and Bladder- decreased urine output
Addictions-
non smoker
Alcohol + but stopped since 3 years
Vitals:
Temp- 97.7F
BP- 160 / 90 mmhg
PR- 98 bpm
RR- 24 cpm
Spo2-98%
GRBS- 184 mg/dl
O/E-
Pallor +
Edema + pitting type (anasarca)
No Icterus, cyanosis, clubbing, lymphadenopathy.
CVS- S1 S2 +
RS- BAE+ crepts +
Dyspnea +
Wheeze +
P/A- distended, non tender
Free fluid +
CNS- NAD
Investigations:
Hb-9.4
TLC- 6000
PLC- 2.09 lakhs
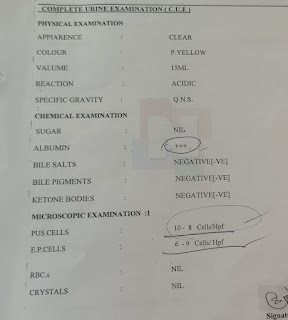
CUE:
Alb- +++
Sug- trace
PC- 3-5
EC- 2-4
RBS- 184 mg/dl
HbA1C- 6.7 %
Urea-139
Creat-5.3
Uric acid-5.8
Na-141
K-5.6
Cl-101
TB- 0.94
DB- 0.13
AST- 10
ALT- 09
ALP- 308
TP-5.1
Alb- 2.5
A/G- 1.02
ABG
PH- 7.124
pCo2- 29.4
PO2- 116
HCO3- 9.3
Spot Urine protein creat ratio- 4.97
Serum LDH- 632
Urinary Na- 198
Urinary K- 16.5
Urinary Cl- 409
HIV, HbSAg, HCV, RAT for COVID 19- negative
ECG:
X Ray chest:
Rt sided pleural effusion with consolidation.

2D echo:
Global hypokinesia
EF- 32%
Severe LV dysfunction
Dilated all chambers
IVC dilated ( 2.25 cms )
USG :
RT gross pleural effusion
Lt moderate pleural effusion
Gall bladder sludge +
B/L grade II RPD
Moderate ascites.
Diagnosis:
Acute LVF ( secondary to HTN) on chronic heart failure ( secondary to CAD)
K/c/oChronic kidney disease
K/c/o DM, HTN, CAD.
Treatment:
Fluid restriction
Inj Lasix 40 mg / IV / Stat followed by inj Lasix 20 mg @ 2.5 ml / hr
Inj Pantop 40 mg IV/OD
Inj Zofer 4 mg IV/SOS
Nebulisation with duolin and budecort 8th hourly
Tab Ecosprin AV ( 75/ 20 ) PO/ H/S
Tab Amlong 10 mg PO/ H/S
Inj HAI S/C pre meal acc to sliding scale
Weight monitoring daily
Foleys catherisation done
Pleural tap done I/v/o Rt sided gross pleural effusion
Pleural fluid analysis:


Post pleural tap chest X Ray

I/o -50/400 ml .
Plan - Hemodialysis in view of Severe metabolic acidosis
And hyperkalemia ( serum K -6 )
Hemodialysis was done for 3 hours
Ultrafiltrate removed- 500 ml
Day 3:
AMC bed 7, Unit 1
65/M
Day 3
S:
SOB decreased
EDEMA decreased
No fever spikes.
Didn't pass stools.
1serial HD done.
O:
Pt is c/c/c
Temp-98.4f
Bp: 130/70mmhg
PR: 84 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA,ISA.
P/A: soft,non tender
GRBS: 176 mg/dl
I/O: 450/350ml
SPO2: 95%
CNS: HMF INTACT
ABG:
PH: 7.243
PCO2: 33.8
PO2: 134
HCO3: 14.0
HEMOGRAM:
HB: 8.4
TC: 7000
PLT: 1.40
RFT:
UREA: 74
CREATININE: 3.1
UA: 3.3
Ca: 7.0
Po4: 3.4
Na: 148
K: 3.4
Cl: 102
LFT:
TB: 0.56
DB: 0.20
AST: 10
ALT: 11
ALP: 133
TP: 3.1
ACB: 1.5
A/G ratio : 0.91

A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVING).
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Pantop 40mg /i.v/od
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
Tab Shelcal PO/OD
Plan for hemodialysis
AMC bed 7, Unit 1
65/M
Day 4
S:
SOB decreased
EDEMA decreased
No fever spikes.
1 session HD done on 10/11/21
O:
Pt is c/c/c
Temp-99.0F
Bp: 130/80 mmhg
PR: 96 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA,ISA.
P/A: soft,non tender
GRBS: 158 mg/dl
I/O: 700ml/500 ml
SPO2: 98% @ RA
CNS: HMF INTACT


ABG:
PH: 7.278
PCO2: 39.1
PO2: 70.0
HCO3: 17.7
HEMOGRAM:
HB: 7.5
TC: 6,100
PLT: 1.5 lakhs
RFT:
UREA: 73
CREATININE: 3.3
UA: 3.6
Ca: 7.6
Po4: 3.4
Na: 148
K: 4.0
Cl: 101
A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVING).
With ANEMIA
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
Tab Shelcal PO/OD
AMC bed 7, Unit 1
65/M
Day 5
S:
SOB decreased
EDEMA decreased
No fever spikes.
2 sessions of hemodialysis done
O:
Pt is c/c/c
Temp-97.6F
Bp: 110/90 mmhg
PR: 82 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA. Coarse crepts + in RT ISA and MSA
P/A: soft,non tender
GRBS: 110 mg/dl
I/O: 900ml/550 ml
SPO2: 98% @ 4L O2
CNS: HMF INTACT
ABG:
PH: 7.323
PCO2: 38.3
PO2: 85.8
HCO3: 19.3

A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVING).
With ANEMIA
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
Tab Shelcal 500 mg PO/OD
AMC bed 7, Unit 1
65/M
Day 6
S:
Facial puffiness +
Pedal edema +
SOB decreased
No fever spikes.
2 sessions of hemodialysis done
O:
Pt is c/c/c
Temp-98.4F
Bp: 130/70 mmhg
PR: 98 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA and ISA
P/A: soft,non tender
GRBS: 164 mg/dl
I/O: 800ml/950ml
SPO2: 98% @ 4L O2
CNS: HMF INTACT
ABG:
PH: 7.285
PCO2: 43.3
PO2: 127
HCO3: 19.9
HEMOGRAM
Hb-7.0
TLC-5,700
PLC-1.5 lakhs
RFT
Urea-97
Creat -4.1
UA-4.7
CA-8.0
PO4-3.8
Na-148
K-4.1
Cl-103

A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVED)
With ANEMIA
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
Tab Shelcal PO/OD
Plan for hemodialysis with PRBC transfusion
AMC bed 7, Unit 1
65/M
Day 7
S:
Pedal edema +
Facial puffiness+
(decreased since yesterday)
SOB decreased
No fever spikes.
1 session of hemodialysis along with PRBC transfusion done yesterday.
Total 3 sessions of hemodialysis done
O:
Pt is c/c/c
Temp-97.7F
Bp: 110/80 mmhg
PR: 99 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA and ISA
P/A: soft,non tender
GRBS: 166 mg/dl
I/O: 1100ml /1000ml
SPO2: 99% @ RA
CNS: HMF INTACT
ABG:
PH: 7.26
PCO2: 56.4
PO2: 78.2
HCO3: 24.7
HEMOGRAM
Hb-8.7
TLC-5,500
PLC-1.34 lakhs
RFT
Urea-55
Creat -2.8
UA-3.3
Ca-9.8
PO4-3.0
Na-148
K-4.0
Cl-99
A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVED)
With ANEMIA
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
AMC bed 7, Unit 1
65/M
Day 8
S:
Pedal edema +
Facial puffiness decreased
SOB decreased
No fever spikes.
3 sessions of hemodialysis and 1 PRBC transfusion done
O:
Pt is c/c/c
Temp-98.6F
Bp: 110/70 mmhg
PR: 86 Bpm regular, normal volume.
CVS: S1S2+, no murmers.
RS: NVBS+ , DECREASED BREATHSOUNDS IN RT IAA and SSA
P/A: soft,non tender
GRBS: 155 mg/dl
I/O: 600 ml/ 800 ml
SPO2: 99% @ 4L O2
CNS: HMF INTACT
ABG: report pending
HEMOGRAM
Hb-7.4
TLC-4,900
PLC-1.25 lakhs
RFT
Urea-53
Creat -2.8
UA-3.0
Ca-8.2
PO4-2.3
Na-149
K-3.3
Cl-105
A:
ACUTE LVF ( secondary to HTN) ON CHRONIC HEART FAILURE (secondary to CAD).
with k/c/o CVA,CKD since 1yr
HTN since 1 and half yr
DM since 3yrs
With RIGHT SIDED PLEURAL EFFUSION ( TRANSUDATIVE)
With REFRACTORY METABOLIC ACIDOSIS ( RESOLVING)
with REFRACTORY HYPERKALEMIA ( RESOLVED)
With ANEMIA
P:
Salt restriction < 2.4 gm/day
fluid restriction < 1lit/day
Inj. Lasix 40mg/i.v / TID
Inj.HAI PRE MEAL
8AM - 2PM - 8PM
Inj. Iron sucrose 1amp in 100ml
Inj Erythropoietin SC/ weekly once
Nebulisation with duolin and budecort
Tab Amlong 10 mg PO H/S
Tab Ecosprin AV ( 75/20) PO/H/S
Tab Met XL 50 mg PO/OD
Tab Metolazone 10 mg PO/BD
Comments
Post a Comment